
Imagine this: you just had a serious medical procedure. Your doctor has recommended follow-up rehabilitation at a specialized facility. You’ve paid your premiums faithfully all year. Then comes the letter – your Medicare Advantage plan has denied the claim. Sound familiar? You’re not alone.
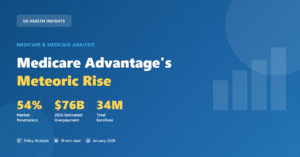
More than 34 million Americans are currently enrolled in Medicare Advantage (MA) plans. While many seniors sign up expecting seamless, affordable coverage, thousands find themselves stuck with plans that deny care, restrict providers, or leave them with sky-high out-of-pocket bills.
In this comprehensive guide, we break down the worst Medicare Advantage plans – what makes a plan bad, which insurers have earned the lowest ratings, what red flags to watch for, and how to protect yourself during open enrollment. Whether you’re choosing a plan for the first time or reconsidering your current coverage, this is the guide you need.
What Makes a Medicare Advantage Plan ‘The Worst’?
Not all Medicare Advantage plans are created equal. The quality gap between the best and worst plans is staggering and it can directly impact your health and financial wellbeing. Experts and regulators use several key indicators to identify low-quality plans.
1. Low CMS Star Ratings
Every year, the Centers for Medicare & Medicaid Services (CMS) rates Medicare Advantage plans on a 1-to-5-star scale. Plans are judged on customer service, member experience, preventive care, chronic disease management, and drug plan performance.
The concerning trend: The average star rating (weighted by enrollment) fell from 4.14 in 2023 to 4.04 in 2024. For 2025, CMS flagged eight contracts with a ‘low performing’ icon — up from six the year before. Seven of those eight were Medicare Advantage plans.
Red Flag: Any plan with 3 stars or below should be approached with extreme caution. CMS considers plans with consistently low ratings as failing to meet quality benchmarks.
2. High Prior Authorization Denial Rates
Prior authorization (PA) is the process where your insurer must approve a service or medication before you receive it. While Original Medicare requires PA for only a limited set of services, Medicare Advantage plans routinely require it for far more and deny it far too often.
Key data point: According to KFF, nearly 53 million prior authorization requests were submitted to Medicare Advantage insurers in 2024, and 4.1 million – roughly 7.7% were denied outright.
What’s alarming is that when denied patients appeal these decisions, they succeed over 80% of the time. This suggests many initial denials are inappropriate — and the worst plans use denials as a cost-cutting tool at patients’ expense.
3. Poor Member Satisfaction Scores
The 2025 J.D. Power Medicare Advantage Study surveyed nearly 11,000 enrollees and found that overall satisfaction dropped 29 points to just 623 out of 1,000 – the steepest decline in the study’s 11-year history. The primary driver? A 39-point collapse in member trust.
- Only 38% of first-year members say their plan fulfills their service expectations
- Common complaints include confusing explanation of benefits, difficulty finding in-network doctors, and prior authorization delays
- Highmark New York ranked as the lowest-rated plan for customer satisfaction in 2025
4. Narrow Provider Networks
Restricted networks are a hallmark of low-quality Medicare Advantage plans. Unlike Original Medicare – where you can see any provider that accepts Medicare anywhere in the country – MA plans typically limit you to an approved network. The worst plans have narrow networks that exclude major hospitals or specialists you depend on.
If your preferred doctor or hospital is suddenly out of network which happens more often than you’d think, since networks change annually – you either pay out-of-pocket or switch providers.
5. Hidden Out-of-Pocket Costs
The maximum out-of-pocket limit for in-network care in 2026 is $9,250 and that doesn’t include prescription drug costs. Prescription costs are separately capped at $2,100 in 2026. The worst plans are structured so that beneficiaries hit these limits quickly, especially for serious or chronic conditions.
The fine print matters: Plans advertise $0 premiums but fail to disclose high copays, strict prior authorization rules, or the cost of out-of-network emergencies.
Major Insurers With Declining Ratings in 2025–2026
While individual plan performance varies by region, several major national carriers have seen notable declines in quality metrics. Here’s what the data reveals:
UnitedHealthcare
CMS 2025 Star Rating: Average 3.5–4.0 across contracts, with a year-over-year decline of 0.39 stars — worse than the industry average.
Enrollment: UnitedHealthcare is the largest Medicare Advantage insurer with 9.9 million members in 2025.
Despite its massive scale, UnitedHealthcare has faced scrutiny for prior authorization denials and network changes. Its stock fell approximately 36% year-to-date as of December 2025, reflecting financial pressures that can translate to benefit cuts.
- Announced plans to scale back Medicare Advantage offerings in 2026
- Engaged in legal disputes with CMS over star rating methodologies
- Members in some regions reported unexpected network changes mid-year
Humana
Star Rating Drop: Humana saw the largest average star rating decline among the top 15 plans — a drop of 0.74 stars — representing a significant quality erosion.
Humana has cut supplemental benefits in recent years to manage rising medical costs. While it has stabilized some offerings for 2026, the insurer’s stock also declined significantly, and the company announced plans to scale back its MA footprint.
- Cut dental, vision, and hearing benefits in multiple markets
- Increased prior authorization requirements for certain services
- Members auto-transferred to different plans due to consolidations
Centene
Prior Authorization Concern: Centene had one of the highest prior authorization denial rates among major Medicare Advantage insurers, according to Kiplinger. While its appeals overturn rate was high (93.6%), this means a huge proportion of initial denials were likely inappropriate.
With only about 1.1 million MA enrollees and a 2% market share, Centene’s outsized denial rate makes it particularly concerning for the seniors who depend on it.
CVS Health / Aetna
CMS Star Ratings: Most Aetna plans are rated 3–4 stars. CVS Health had the second-highest prior authorization denial rate among major insurers, with 89.7% of its appealed denials overturned — again suggesting many denials were unwarranted.
With a 12% market share and 4.1 million enrollees, even a fraction of unnecessary denials affects hundreds of thousands of Americans.
Zing Health
Among smaller plans, Zing Health had one of the lowest-performing contracts in the 2025 CMS star ratings — a warning sign for members in markets where Zing operates.
Highmark New York
According to the 2025 J.D. Power study, Highmark New York ranked dead last for member satisfaction in its market — a distinction no plan wants and no enrollee deserves.
Red Flags That Identify the Worst Medicare Advantage Plans
So how do you spot a bad Medicare Advantage plan before you’re locked into it? Here are the red flags that consumer advocates and healthcare experts say to watch closely:
- Low CMS Star Rating (below 3.5 stars): CMS publishes star ratings every fall before open enrollment. Plans with 3 stars or below are consistently underperforming on care quality and member satisfaction.
- High prior authorization requirements: Plans that require prior authorization for a long list of routine services create unnecessary barriers to care. Review a plan’s prior authorization list before enrolling.
- Very narrow provider networks: If your current doctors aren’t in-network, that’s a serious problem. Always check the plan’s provider directory and verify independently, since directories are often outdated.
- Annual benefit reductions: Plans that keep cutting dental, vision, hearing, or prescription benefits year after year are prioritizing profits over patient care.
- High out-of-pocket maximums: In 2026, the maximum is $9,250 for in-network care. Plans near that ceiling offer less financial protection than they appear to.
- Confusing or misleading marketing: CMS has reported double-digit increases in complaints about misleading Medicare Advantage marketing. Watch for promises of ‘free’ coverage that ignores copays and restrictions.
- Frequent plan consolidations: If a plan keeps merging with others or exiting markets, your coverage and providers could change without warning.
- No or minimal digital tools: The J.D. Power study found that digital satisfaction among the highest-performing plans was 98 points higher than among the lowest-performing ones. Poor digital tools signal poor member support overall.
The Prior Authorization Crisis: By the Numbers
Prior authorization has become the single biggest pain point for Medicare Advantage members and the statistics are alarming.
53 million prior authorization requests were submitted in 2024 alone.
4.1 million (7.7%) of those requests were denied – up from under 6% in 2019–2021.
Over 80% of appealed denials are overturned – suggesting widespread inappropriate denials.
Only ~10% of denied patients even bother to appeal – leaving millions without the care they’re entitled to.
73% of Americans say delays and denials of care by health insurers are a ‘major problem,’ according to a 2025 KFF poll.
47% of people who needed prior authorization found the process ‘somewhat’ or ‘very’ difficult to navigate.
The most troubling finding: When Medicare Advantage denials are appealed, they’re overturned 82% of the time. In traditional Medicare, only 29% of appealed denials are overturned. This gap suggests that MA plans are systematically over-denying care.
The Senate Homeland Security Committee’s investigative subcommittee has scrutinized large Medicare Advantage insurers specifically for their high rates of prior authorization denials for post-acute care – like skilled nursing facilities and inpatient rehabilitation – services that are critical for seniors recovering from surgery or illness.
How to Evaluate and Compare Medicare Advantage Plans
The good news: you have more tools than ever to research plans before committing. Here’s a step-by-step framework:
Step 1: Check the CMS Star Rating
Visit Medicare.gov and use the Plan Finder tool. Filter by star ratings. Aim for plans with 4 stars or above. Five-star plans have the added bonus of being available for enrollment year-round.
Step 2: Verify Your Doctors Are In-Network
Don’t rely solely on the plan’s online directory. Call your doctor’s office directly and ask whether they accept the specific Medicare Advantage plan you’re considering — including the specific contract number if possible.
Step 3: Review the Prior Authorization List
Starting in 2026, Medicare Advantage insurers are required to publish a list of all services requiring prior authorization, along with their approval and denial rates. Review this carefully, especially if you have chronic conditions or anticipate surgeries or specialist care.
Step 4: Calculate Your True Costs
Add up the monthly premium plus the expected copays for the services you use most. Compare the total cost – not just the premium against Original Medicare plus a Medigap supplement plan.
Step 5: Check Drug Coverage
Ensure your specific medications are on the plan’s formulary. Drug plan deductibles can be no higher than $615 in 2026, and out-of-pocket prescription costs are capped at $2,100 for 2026. Verify that your drugs are in the lowest possible tier.
Step 6: Read the Annual Notice of Change (ANOC)
Your current plan must send you an ANOC by September 30 each year. This document spells out every change to your benefits, costs, and network for the coming year. Read it carefully and if anything significant has changed, it’s time to compare alternatives during Open Enrollment (Oct 15 – Dec 7).
When to Switch Away From Your Medicare Advantage Plan
You don’t have to stay in a bad plan. Here are the most important times when you can make a change:
- Annual Open Enrollment (October 15 – December 7): You can switch to any Medicare Advantage plan or return to Original Medicare. Changes take effect January 1.
- Medicare Advantage Open Enrollment (January 1 – March 31): If you’re already in an MA plan and unhappy, you can switch to another MA plan or return to Original Medicare during this window.
- Special Enrollment Periods (SEPs): If your plan leaves your area, loses its Medicare contract, or if you move, you may qualify for a Special Enrollment Period to switch plans outside the normal window.
- 5-Star Enrollment: Five-star plans can be joined at any time during the year – a major advantage if you miss open enrollment.
Important: Switching from Medicare Advantage back to Original Medicare may be difficult if you have pre-existing conditions and want to buy a Medigap supplement policy. In most states, Medigap insurers can use medical underwriting outside of specific guaranteed issue windows. Consider this carefully before switching.
Medicare Advantage vs. Original Medicare: The Real Comparison
For many seniors, especially those with complex health needs, Original Medicare paired with a Medigap supplement plan provides superior protection. Here’s a quick comparison:
Provider Access: Original Medicare allows you to see any provider that accepts Medicare nationwide. Medicare Advantage restricts you to an in-network panel.
Prior Authorization: Original Medicare requires PA for a small set of services. Medicare Advantage can require PA for a far broader list.
Travel Coverage: Original Medicare covers you across all 50 states. Most Medicare Advantage plans only cover emergency care outside their service area.
Out-of-Pocket Predictability: Medigap plans can cover nearly all of Original Medicare’s cost-sharing, offering far more financial predictability than MA plans.
Extra Benefits: Medicare Advantage plans often include dental, vision, and hearing. Original Medicare does not – though standalone plans are available.
The bottom line: if your priority is access to any doctor, minimal paperwork, and predictable costs – especially if you have serious or complex health needs – Original Medicare with Medigap may serve you better than the average Medicare Advantage plan.
Take Action Before Open Enrollment Closes
Don’t wait until you’re denied care to realize your plan isn’t working for you. Take these steps today:
- Visit Medicare.gov/plan-compare to check your plan’s star rating
- Call 1-800-MEDICARE (1-800-633-4227) for free, unbiased assistance
- Contact your State Health Insurance Assistance Program (SHIP) for personalized guidance at no cost
- Report misleading marketing or wrongful denials to 1-800-MEDICARE or your State Senior Medicare Patrol (SMP)
Frequently Asked Questions (FAQ)
Q: How do I find out if my Medicare Advantage plan is rated poorly?
Visit Medicare.gov and use the Medicare Plan Finder. Every plan shows its CMS star rating from 1 to 5 stars. Plans rated 3 stars or below are considered low-performing. You can also view ‘low performing’ icons on the Plan Finder for plans that have consistently failed quality benchmarks.
Q: Which Medicare Advantage plan has the most complaints?
Complaint data varies by region, but national data from J.D. Power’s 2025 study identified Highmark New York as the lowest-ranked plan for member satisfaction. CMS also maintains a low-performing plan list with eight contracts flagged for 2025 – primarily Medicare Advantage plans. Centene and CVS Health/Aetna also drew attention for high prior authorization denial rates.
Q: Can I switch out of a bad Medicare Advantage plan mid-year?
In most cases, you can only switch during the Annual Open Enrollment Period (October 15 – December 7) or the Medicare Advantage Open Enrollment Period (January 1 – March 31). However, certain life events – like moving, losing other coverage, or your plan losing its Medicare contract – may qualify you for a Special Enrollment Period that allows mid-year changes.
Q: What happens if my Medicare Advantage plan denies a claim?
You have the right to appeal. Request a written denial notice if you haven’t received one, then file a formal appeal with your plan. If the plan upholds the denial, you can escalate to an independent review entity. Statistics show that over 80% of appeals are successful, so it is absolutely worth fighting an unjust denial. Contact 1-800-MEDICARE or your SHIP counselor for free help navigating the appeals process.
Q: Is Original Medicare better than Medicare Advantage?
It depends on your individual health needs, finances, and priorities. Original Medicare offers nationwide provider access with no network restrictions and minimal prior authorization requirements. Paired with a Medigap supplement plan, costs become highly predictable. Medicare Advantage can offer lower premiums and extra benefits like dental and vision, but often comes with restricted networks, prior authorization hurdles, and less financial predictability. For those with complex or chronic health conditions, Original Medicare with Medigap is often the safer choice.
Q: What is the out-of-pocket maximum for Medicare Advantage in 2026?
The in-network out-of-pocket maximum for Medicare Advantage plans in 2026 is $9,250. Note that prescription drug costs are handled separately and are capped at $2,100 in 2026. Out-of-network costs may be even higher, depending on your plan type.
Q: How do I report a bad Medicare Advantage plan or misleading marketing?
You can file a complaint directly with CMS by calling 1-800-MEDICARE (1-800-633-4227), available 24/7. You can also contact your State Health Insurance Assistance Program (SHIP), file a complaint with your state insurance department, or report suspected fraud or abuse to your regional Senior Medicare Patrol (SMP).
Q: Do Medicare Advantage plans get worse every year?
Not necessarily, but the trend is concerning. Average star ratings have declined for several consecutive years, and member satisfaction hit a multi-year low in 2025. Several major insurers have scaled back benefits and narrowed networks to manage costs. The landscape is changing rapidly, which makes it more important than ever to review your plan each year during Open Enrollment rather than simply auto-renewing.
Final Thoughts: Your Coverage, Your Health, Your Choice
Medicare Advantage is not inherently bad but the worst plans can genuinely put your health and finances at risk. Low star ratings, aggressive prior authorization denials, narrow networks, and misleading marketing are real problems that affect millions of Americans every year.
The good news is that you have the power to make an informed choice. Use the tools available to you CMS star ratings, J.D. Power satisfaction scores, prior authorization transparency data, and free counseling through SHIP to evaluate every plan on its actual merits, not just its marketing.
Your health is too important to leave to chance or a slick advertisement. Review your plan annually, know your rights, and don’t hesitate to switch if your plan isn’t serving you well.

No comment yet, add your voice below!