Every day, a mid-sized hospital generates roughly 50 petabytes of data from EHR entries and lab results to insurance claims and imaging files. Yet most health systems can only use a fraction of it. Not because the data isn’t there. Because it’s stored in the wrong place, in the wrong format, for the wrong purpose.
Here’s a scenario you’ve probably seen or lived:
A quality improvement team wants to analyze readmission trends across three hospitals. But one facility runs Epic, another runs Cerner, and the third uses a legacy system built in 2003. The data exists but it lives in separate healthcare databases that weren’t designed to talk to each other. No one can run a cross-system query without a two-month IT project.
That’s not a data problem. That’s an infrastructure decision problem.
At the heart of it is a question most healthcare organizations eventually have to face: Do we need a healthcare database, a data warehouse, or both and what’s actually the difference?
This guide cuts through the confusion. Whether you’re a health IT leader evaluating your next infrastructure investment, a clinical informatics director trying to make sense of your current stack, or a digital health executive building a platform from scratch — this is the definitive breakdown you’ve been looking for.
What is a Healthcare Database?
A healthcare database is a structured, transactional data system designed to capture, store, and retrieve patient and operational data in real time or close to it. It’s the engine running behind most clinical software you interact with daily.
When a nurse documents a medication administration in an EHR, when a front desk team checks a patient in for an appointment, when a billing system generates a claim after a visit – all of that happens inside a healthcare database.
Core Characteristics of Healthcare Databases
- Transaction-first design: Built for CRUD operations (Create, Read, Update, Delete) at high speed and volume.
- Normalized data structure: Data is organized to reduce redundancy and support fast read/write performance.
- Real-time or near-real-time access: Clinicians see current patient information, not yesterday’s snapshot.
- Point-of-care optimization: Designed to support individual patient workflows, not population-level analysis.
- HIPAA compliance infrastructure: Built-in access controls, audit logs, and encryption to protect Protected Health Information (PHI).
Common Examples of Healthcare Databases
- Electronic Health Record (EHR) systems: Epic, Oracle Cerner, MEDITECH, athenahealth – each running on a relational database backend (often Oracle, Microsoft SQL Server, or PostgreSQL).
- Practice Management Systems (PMS): Handle scheduling, registration, and billing data.
- Laboratory Information Systems (LIS): Track specimen processing, test orders, and results.
- Pharmacy Information Systems: Manage drug dispensing records and clinical decision support.
- Picture Archiving and Communication Systems (PACS): Store and retrieve medical imaging data.
- Health Information Exchanges (HIEs): Connect databases across organizations for real-time data sharing.
What Healthcare Databases Are Great At
Healthcare databases shine when the task is operational: pulling up a patient chart, checking a medication history, processing a claim, or scheduling a follow-up. Their architecture is specifically optimized for these rapid, record-by-record interactions.
💡 Think of a healthcare database like a busy hospital unit. Everything is happening in real time. Orders are written, medications are given, vital signs are charted – it’s all immediate, individual, and constantly changing.
What Is a Healthcare Data Warehouse?
A healthcare data warehouse (HDW) is an analytical data repository designed to consolidate, standardize, and store large volumes of historical data from multiple source systems for the purpose of reporting, analytics, and strategic decision-making.
Unlike a transactional database, a data warehouse isn’t being updated by clinicians in real time. Instead, data from EHRs, billing systems, claims processors, lab systems, and other sources is extracted, transformed, and loaded (ETL) into the warehouse on a scheduled basis – daily, hourly, or in some architectures, in near-real-time.
Core Characteristics of Healthcare Data Warehouses
- Subject-oriented: Organized around key healthcare domains like patients, encounters, diagnoses, procedures, and costs – not around individual applications.
- Integrated: Combines data from disparate source systems into a single, consistent schema.
- Time-variant: Preserves historical snapshots so analysts can track trends across months and years.
- Non-volatile: Once loaded, data is generally not deleted or modified – it’s a stable analytical record.
- Optimized for queries: Uses columnar storage, indexing, and aggregation to support complex analytical queries across millions of records.
Common Examples and Technologies
- Enterprise data warehouses (EDW): Centralized platforms deployed by large health systems often built on Amazon Redshift, Google BigQuery, Microsoft Azure Synapse, Snowflake, or IBM Db2 Warehouse.
- Departmental data marts: Smaller, domain-specific warehouses (e.g., a finance data mart or a quality reporting mart) that may feed from or into a broader EDW.
- Clinical data repositories (CDRs): Specialized warehouses that aggregate longitudinal patient data for population health and quality analytics.
- Claims data warehouses: Used by payers and ACOs to analyze utilization, cost trends, and care gaps at scale.
What Data Warehouses Are Great At
Data warehouses are purpose-built for analytical thinking at scale. They answer questions like:
- What is our 30-day readmission rate across all facilities for heart failure patients in Q1 2026 vs. Q1 2025?
- Which providers have the highest average cost-per-episode for knee replacement, and how does that correlate with outcomes?
- Where are our biggest care gaps in the diabetic population enrolled in our value-based care program?
- How does our HEDIS performance compare across payer contracts?
These are not questions a transactional EHR database can answer quickly. A data warehouse can.
💡 Think of a healthcare data warehouse like the hospital’s administrative suite. Quieter than the unit floor, but that’s where the strategic analysis happens reviewing patterns, identifying trends, planning for the future.
Healthcare Database vs Data Warehouse: A Side-by-Side Comparison
| Factor | Healthcare Database | Healthcare Data Warehouse |
|---|---|---|
| Primary Purpose | Transactional operations & real-time data capture | Historical analysis & strategic reporting |
| Data Structure | Normalized (3NF) for fast writes | Denormalized (star/snowflake schema) for fast reads |
| Query Type | Simple, record-level lookups | Complex, multi-table aggregations |
| Data Freshness | Real-time or near real-time | Batch-loaded (hourly/daily/weekly) |
| Users | Clinicians, front desk, billing staff | Analysts, executives, quality teams, actuaries |
| Volume Handled | Millions of transactions | Billions of historical records |
| Data Sources | One application at a time | Multiple integrated source systems |
| Update Frequency | Continuous (every interaction) | Periodic (ETL batch or micro-batch) |
| HIPAA Consideration | PHI at point of care | De-identified or role-based access for analytics |
| Examples | Epic, Cerner, MEDITECH | Snowflake, Azure Synapse, BigQuery, Redshift |
| Optimization | Write performance | Read/query performance |
| Historical Depth | Limited (current state focus) | Years of longitudinal data |
The Architecture Behind Healthcare Data Infrastructure
Understanding the difference between a database and a data warehouse becomes much clearer when you see how they fit together in a modern health system’s data architecture.
The Traditional Three-Tier Model
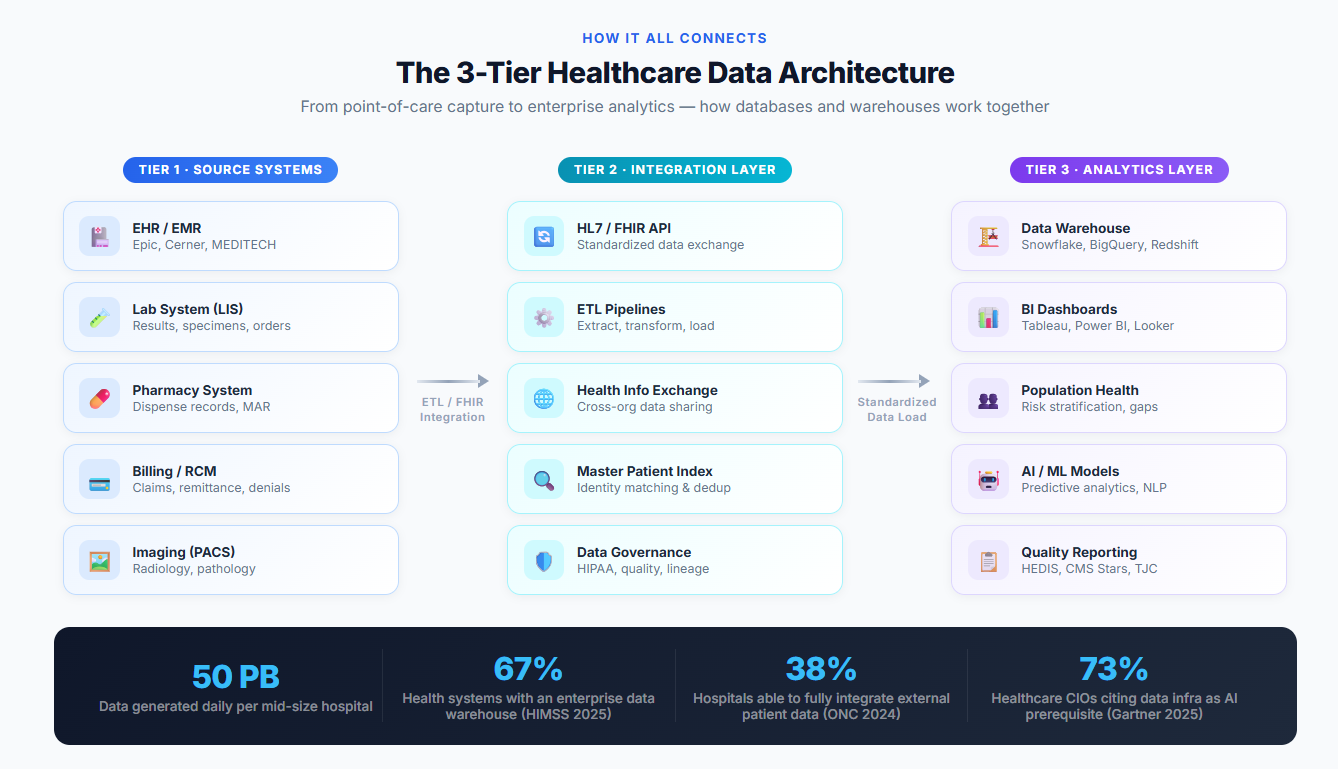
Tier 1 — Source Systems (Databases): EHRs, billing systems, lab systems, pharmacy systems, and other operational tools each maintain their own transactional databases. These are the point-of-care systems clinicians use every day.
Tier 2 — Integration & ETL Layer: Data from Tier 1 is extracted, cleaned, standardized (often to common data models like OMOP CDM, HL7 FHIR, or PCORnet), and loaded into a central repository. This is where Health Information Exchanges (HIEs), integration engines (like Rhapsody, Mirth Connect, or Azure API for FHIR), and ETL pipelines live.
Tier 3 — Data Warehouse / Analytics Layer: The standardized data lands in a warehouse where analysts, quality teams, and executives run reports, dashboards, and population health models.
The Modern Data Lakehouse Approach
Many forward-thinking health systems are now adopting a data lakehouse architecture — a hybrid that combines the flexibility of a data lake (raw, unstructured storage) with the query performance of a data warehouse.
Platforms like Databricks Delta Lake and Snowflake enable health systems to:
- Store raw HL7 FHIR messages, clinical notes, imaging metadata, and genomic data in their native formats
- Apply structure and schema-on-read for analytical workloads
- Support both batch analytics and real-time streaming use cases from a single platform
Key Stat: According to a 2025 HIMSS report, 67% of health systems now report operating a formal enterprise data warehouse, up from 52% in 2021 with the majority planning to migrate toward cloud-native platforms within the next three years.
Real-World Use Cases: When to Use Each
Use Cases That Require a Healthcare Database
1. Clinical Documentation A physician documents a patient encounter in Epic. The EHR writes that data into its relational database instantly – accessible to the nurse, pharmacist, and billing team in seconds. This requires a transactional database. No warehouse can support this workflow.
2. Real-Time Clinical Decision Support When a provider orders a medication contraindicated with another drug the patient is taking, the EHR fires an alert. That alert fires based on live data in the clinical database – not a yesterday’s batch load.
3. Appointment Scheduling and Registration Booking a patient appointment, checking insurance eligibility, and registering a new patient all require real-time read/write access to operational databases.
4. Revenue Cycle Management Claims generation, remittance posting, and denial tracking happen inside the billing system’s transactional database – requiring immediate, record-level accuracy.
5. HIPAA-Compliant PHI Storage The canonical record of protected health information – the legal medical record lives in the source EHR database, not in an analytics warehouse.
Use Cases That Require a Healthcare Data Warehouse
1. Population Health Management A health plan wants to identify members with uncontrolled diabetes who haven’t had an A1C test in 12 months. That query requires aggregating data across millions of claims and clinical records over multiple years – a textbook data warehouse use case.
2. Quality Reporting (HEDIS, CMS Stars, Joint Commission) Healthcare organizations must report on dozens of quality measures annually. Generating these reports requires pulling structured historical data from across the enterprise – something a data warehouse does in minutes that would otherwise take analysts weeks.
3. Value-Based Care Analytics Under ACO and value-based care contracts, health systems need to understand total cost of care per patient, risk stratification scores, and care gap closure rates. These analyses require cross-system, longitudinal data – exactly what a data warehouse provides.
4. Financial Forecasting and Cost Analytics CFOs and finance teams use data warehouses to model revenue trends, forecast payer mix changes, and analyze cost variances by service line, facility, or provider.
5. Research and Clinical Trials Academic medical centers use enterprise data warehouses often built on OMOP or i2b2 frameworks — to identify eligible research cohorts, analyze outcomes, and support FDA submissions.
6. Operational Efficiency and Supply Chain Analyzing OR utilization, bed occupancy, supply consumption, and staffing ratios requires historical operational data – another strong data warehouse use case.
Key Challenges in Healthcare Data Management
The Interoperability Problem
Despite years of progress, healthcare data still lives in siloed systems across most organizations. A 2024 ONC report found that only 38% of hospitals were able to electronically send, receive, and integrate patient data from outside providers without any manual intervention.
This is the fundamental driver for data warehousing in healthcare – the need to create a unified view of the patient across systems that don’t naturally talk to each other.
HIPAA Compliance at Every Layer
Both healthcare databases and data warehouses must comply with the HIPAA Privacy Rule and Security Rule. However, they present different compliance challenges:
- Databases must enforce role-based access at the point of care, audit every PHI access, and maintain data integrity.
- Data warehouses often use de-identification or limited data sets to enable broader analytical access while reducing PHI exposure risk. The Safe Harbor method and Expert Determination method are the two HIPAA-recognized de-identification approaches.
Data Quality and Governance
A data warehouse is only as good as the data fed into it. Common data quality issues in healthcare include:
- Inconsistent coding practices (ICD-10, CPT, NDC codes applied differently across facilities)
- Duplicate patient records across systems (master patient index failures)
- Incomplete documentation in free-text clinical notes
- EHR data that reflects billing optimization rather than clinical accuracy
Without a robust data governance framework — including data stewardship, lineage tracking, and quality monitoring – a healthcare data warehouse quickly becomes an expensive source of unreliable reports.
Legacy System Integration
Many health systems still operate legacy databases – some running on infrastructure from the 1990s or early 2000s. Integrating these systems into modern analytics pipelines requires significant investment in middleware, API development, and often custom ETL work.
Healthcare Data Warehouse vs Database: The Compliance Lens
From a regulatory standpoint, both systems carry significant compliance obligations, but they differ in scope and approach.
For Healthcare Databases:
- Must implement access controls limiting PHI access to the minimum necessary
- Must maintain audit logs of all PHI access and modifications
- Must encrypt data at rest and in transit
- Must have disaster recovery and backup procedures
- Must conduct regular risk assessments under the HIPAA Security Rule
For Healthcare Data Warehouses:
- De-identification reduces some HIPAA obligations but introduces data governance complexity
- Business Associate Agreements (BAAs) required with any cloud vendor processing PHI
- Must enforce role-based access controls aligned with job function
- Must address data lineage — knowing exactly where every piece of data came from and how it was transformed
- Subject to 42 CFR Part 2 restrictions for substance use disorder data, even in aggregate analytics
Emerging Trends Reshaping Healthcare Data Infrastructure in 2026
1. Real-Time Analytics and Streaming Architectures
The gap between databases and warehouses is narrowing. Platforms like Apache Kafka, Azure Event Hubs, and Snowflake Unistore now support streaming data pipelines that feed near-real-time clinical data into analytical systems. This enables use cases like live sepsis monitoring dashboards and real-time care coordination alerts based on warehouse-level population data.
2. AI and Generative AI Integration
Health systems are increasingly using their data warehouses as the foundation for AI model training – particularly for predictive analytics (readmission risk, deterioration alerts, no-show prediction) and generative AI applications (clinical documentation assistance, prior authorization automation). The quality of the underlying warehouse directly determines the quality of the AI outputs.
Key Stat: A 2025 Gartner survey found that 73% of healthcare CIOs cited “improving data infrastructure” as a prerequisite before deploying clinical AI at scale.
3. FHIR-Native Data Platforms
The HL7 FHIR (Fast Healthcare Interoperability Resources) standard is transforming how healthcare data is stored and exchanged. New FHIR-native data platforms – like Microsoft Azure Health Data Services and Google Cloud Healthcare API allow health systems to query clinical data using FHIR APIs directly from their warehouses, eliminating many traditional ETL steps.
4. Cloud Migration at Scale
On-premise data warehouses are rapidly giving way to cloud-native alternatives. Snowflake, Google BigQuery, and Amazon HealthLake are seeing strong healthcare adoption for their ability to scale elastically, support complex HIPAA compliance frameworks, and integrate with modern analytics and AI tools.
5. Unified Namespace and Federated Data Access
Rather than centralizing all data in a single warehouse, some health systems are adopting data mesh and federated query architectures allowing analysts to query distributed databases as if they were a single unified source, without physically moving data. Tools like Trino (formerly PrestoSQL) and Databricks Unity Catalog are enabling this approach.
How to Choose: Healthcare Database vs Data Warehouse
The honest answer is: most health systems need both. But the decision about where to invest, when to invest, and how much to invest depends on your organization’s current state and strategic goals.
You Need to Prioritize Your Database Infrastructure If:
- Your clinical staff are experiencing EHR performance issues, downtime, or slow documentation workflows
- You’re implementing a new EHR or point-of-care system
- You have gaps in real-time clinical decision support
- Your revenue cycle system has data integrity or performance problems
- You’re dealing with regulatory findings related to PHI access controls or audit logging
You Need to Invest in a Data Warehouse If:
- You’re entering value-based care contracts and need population health analytics
- Your quality team is manually pulling data from multiple systems for reporting
- Your executives don’t have reliable, timely visibility into operational and financial performance
- You’re planning to implement AI or predictive analytics
- You’re operating multiple facilities, EHR platforms, or lines of business that need integrated reporting
The Sweet Spot: A Modern, Integrated Data Strategy
The organizations seeing the greatest impact aren’t choosing one over the other, they’re building integrated data architectures where:
- Transactional databases handle real-time point-of-care needs
- A FHIR-based integration layer standardizes and governs data movement
- A cloud data warehouse (or lakehouse) enables enterprise analytics
- AI/ML models are trained and deployed on top of the warehouse layer
- Insights flow back into point-of-care systems to close the loop
Companies like Curitics Health are building exactly this kind of architecture — offering AI-powered, low-code platforms that unify clinical workflow data with analytical infrastructure, enabling health systems to bridge the gap between operational databases and strategic data warehouses without requiring massive custom engineering projects.
Best Practices for Healthcare Data Infrastructure
1. Adopt a Common Data Model
Standardizing on frameworks like OMOP CDM, PCORnet, or FHIR enables interoperability, research collaboration, and faster integration of new data sources into your warehouse.
2. Invest in Data Governance Before You Scale
Data quality, stewardship, and lineage tracking are non-negotiable. Establish a Data Governance Committee with representatives from IT, clinical informatics, compliance, finance, and operations before expanding your analytics infrastructure.
3. Build for the Cloud From Day One
On-premise warehouses have high maintenance overhead and limited scalability. Cloud-native platforms offer better performance, lower total cost of ownership, and faster time-to-insight for most healthcare organizations.
4. Plan for FHIR Compliance
The ONC’s HTI-1 rule (effective 2024–2026) requires health IT developers and many health systems to support FHIR R4 APIs. Align your data strategy with FHIR now to avoid costly retrofits later.
5. Start With High-Value Analytics Use Cases
Don’t try to boil the ocean. Identify two or three specific analytics use cases with clear ROI — like reducing readmissions, improving HEDIS scores, or reducing claim denials — and build your warehouse infrastructure around delivering those outcomes first.
6. Don’t Forget the Human Layer
Technology is only part of the equation. Health systems that successfully leverage their data infrastructure invest equally in training analysts, empowering clinical informatics teams, and building a data-literate culture among clinical and operational leaders.
FAQ
1. What is the main difference between a healthcare database and a data warehouse?
A healthcare database is designed for real-time transactional operations – like documenting patient care in an EHR or processing a claim. A data warehouse is designed for analytical workloads like reporting on population health trends or measuring quality performance across a health system. Databases optimize for fast writes; warehouses optimize for fast reads across large historical datasets.
2. Can a healthcare organization use a database as a data warehouse?
Technically, you can run reports against a transactional database, but it’s not advisable at scale. Running complex analytical queries against an operational database can severely degrade performance for clinical users – slowing down EHR workflows at the point of care. Purpose-built data warehouses handle analytical queries far more efficiently.
3. What is an example of a healthcare data warehouse?
Common healthcare data warehouse implementations include health systems using Snowflake or Azure Synapse to consolidate Epic and Cerner data for enterprise analytics, payers using Amazon HealthLake for claims and clinical data integration, and academic medical centers using OMOP CDM on PostgreSQL for research cohort identification.
4. How does HIPAA apply to healthcare data warehouses?
HIPAA applies to any system storing or processing Protected Health Information (PHI). Data warehouses are often configured with de-identified or limited data sets to enable broader analytical access, but if PHI is present, all HIPAA Security Rule requirements apply — including access controls, encryption, audit logging, and Business Associate Agreements with any cloud vendors.
5. What is the difference between a clinical data repository and a data warehouse in healthcare?
A clinical data repository (CDR) is a specialized form of data warehouse focused specifically on longitudinal patient clinical data. A broader enterprise data warehouse (EDW) typically includes clinical, financial, operational, and claims data — providing a more complete view of the organization. Many health systems operate both: a CDR for clinical analytics and a broader EDW for enterprise reporting.
6. What is a healthcare data lake vs a data warehouse?
A data lake stores raw, unstructured data — including clinical notes, imaging files, genomic sequences, and HL7 messages — in its native format at low cost. A data warehouse stores structured, processed data optimized for querying. A data lakehouse (increasingly popular in healthcare) combines both: storing raw data at scale while enabling warehouse-speed querying on structured subsets.
7. Do small healthcare organizations need a data warehouse?
Not always in the traditional sense. Smaller practices and community health centers may meet their analytical needs with embedded reporting in their EHR, a data mart (a smaller, domain-specific warehouse), or a cloud-based analytics platform without building a full enterprise data warehouse. However, as organizations grow and enter value-based care arrangements, the need for more robust data infrastructure typically increases.
8. How long does it take to implement a healthcare data warehouse?
Implementation timelines vary widely based on scope, data sources, and organizational readiness. A focused departmental data mart might take 3–6 months. A full enterprise data warehouse integrating multiple EHRs, billing systems, and claims data can take 12–24 months or longer. Cloud-native platforms and pre-built healthcare data models can significantly reduce implementation time.
9. What is OMOP CDM and why does it matter for healthcare data warehouses?
The Observational Medical Outcomes Partnership Common Data Model (OMOP CDM) is an open community standard for organizing healthcare data in a consistent, interoperable format. Standardizing your data warehouse on OMOP enables participation in research networks, makes your data compatible with a large ecosystem of analytical tools, and facilitates benchmarking against peer organizations. It’s widely used in academic medical centers and large health systems.
Final Thoughts: Infrastructure Is Strategy
The divide between healthcare databases and data warehouses isn’t just a technical distinction – it reflects two fundamentally different modes of healthcare delivery: reacting to individual patient needs in real time versus planning and optimizing care for entire populations.
The health systems winning in today’s environment are building architectures that do both. They’re using modern, HIPAA-compliant databases to support seamless point-of-care experiences. And they’re using cloud-native data warehouses and analytics platforms to turn decades of clinical and operational data into actionable intelligence.
The question isn’t really database or warehouse – it’s how do you build an integrated data strategy that serves both your patients today and your population tomorrow?
The organizations that answer that question well will define the standard of care for the next decade.